Iron Overload - The Complications with Body Composition
System Used:
iNSiGHT

A Short Article Review:
Bone loss and the breakdown of bone architecture are key characteristics associated with osteoporosis, leading to an increase in fractures1. Currently, more than 12 million people in North America suffer from osteoporosis and these numbers may quadruple by 20302,3. This staggering number is, and will continue to, lead to a massive financial burden for North America. This is the rationale for continuing to develop preventative methods and treatment options for osteoporosis.
It is well known that iron (Fe) is an essential element in many physiological processes. However, too much of a good thing can lead to a poorer outcome. Excess Fe can generate reactive oxygen species via the Fenton reaction4. This Fe overload is strongly associated with osteoporosis as it inhibits osteogenic differentiation of bone marrow mesenchymal stem cells5. We classify this as ferroptosis, also known as iron-dependent regulated cell death (RCD). Lipid-associated radicals and lipid peroxides are formed during Fe overload leading to ferroptosis. One of the current hallmarks of ferroptosis is glutathione peroxidase 4 (GPX4), as it plays a major role in triggering ferroptosis via its inactivation leading to glutathione (GSH) deficiency6. However, the underlying mechanisms are not well understood within this pathway. If we can better understand the underlying mechanisms, we can generate better therapeutic interventions for osteoporosis associated with Fe overload.
The goal of Yan, Z, and coworkers was to determine if Fe overload could lead to ferroptosis in osteoblast and if this process can be inhibited both in vitro and in vivo7. They used ferric ammonium citrate in their cell model as the iron overload source and used deferoxamine and ferrostatin-1 to inhibit ferroptosis within cells. Their mouse model of iron overload was established with iron dextran for the iron overload source. To determine ferroptosis of osteoblasts in vivo immunohistochemical analysis was performed. Bone formation was measured with enzyme-linked immunosorbent and calcein-alizarin red s labeling. The iNSiGHT Dual x-ray absorptiometry (DXA or DEXA) system was used as a tool in the evaluation of osteoporosis. Micro-computed tomography (μCT) and histopathological analysis were also two additional tools used to evaluate osteoporosis7. I have summarized the results of the effects Fe overload had on various pharmacological functions in the table below.
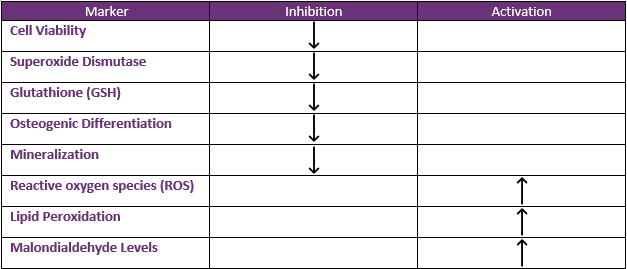
Table 1. Summary of the pharmacological changes that arise due to iron overload.
The authors then found that if they inhibited ferroptosis, they were able to reverse the changes in the above table. This inhibition resulted in improved osteogenesis in vivo using both deferoxamine and ferrostatin-1. With these results, they concluded that ferroptosis plays an essential role in osteoporosis because of Fe overload at a molecular level. The authors also assessed this in an animal model using both µCT and DXA. The DXA results can be seen in figure 1 below. DXA was used to measure the bone mineral density (BMD) for the total animal, as well as regions that are highlighted in the image below (blue for lumbar and red for femur). For a normal wild-type mouse of 12 weeks of age, the BMD should be around 0.50 to 0.60 g/cm2; while in models of osteoporosis, such as that induced by iron overload, the BMD would be expected to decrease, while therapeutic interventions would be aimed to reverse or protect against this decrease8,9.
Thirty-two 12-week-old female C57/BL6 mice were used to assess Fe-overload and treatment with deferoxamine (DFO) and ferrostatin-1 (Fer-1). Female mice were divided into four groups. There was the vehicle group, an iron overload group, a DFO treatment group with iron-dextran (FeDex) injection, and a DFO plus Fer-1 injection group with FeDex injection. After 2 months of this treatment regimen (FeDex once/week, DFO and Fer-1 every 3 days), the lumbar spine BMD, femur BMD, and total BMD were measured with the iNSiGHT DXA system.
Thirty-two 12-week-old female C57/BL6 mice were used to assess Fe-overload and treatment with deferoxamine (DFO) and ferrostatin-1 (Fer-1). Female mice were divided into four groups. There was the vehicle group, an iron overload group, a DFO treatment group with iron-dextran (FeDex) injection, and a DFO plus Fer-1 injection group with FeDex injection. After 2 months of this treatment regimen (FeDex once/week, DFO and Fer-1 every 3 days), the lumbar spine BMD, femur BMD, and total BMD were measured with the iNSiGHT DXA system.
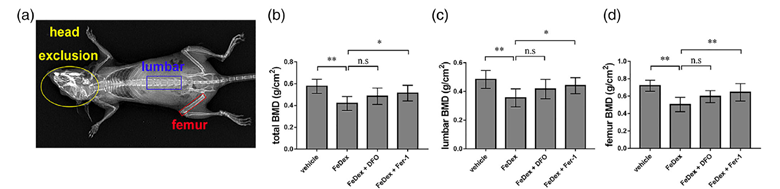
Figure 1. The use of the iNSiGHT DXA system to assess bone mineral density (BMD in g/cm2) in a mouse model of iron overload. A) Digital radioautography image of the mouse with the highlighting of both the lumbar and femur region in which BMD measurements were compared to the whole-body BMD. B-D) BMD measurements for the whole body, lumbar, and femur in a mouse model of iron overload and when treated with either DFO and Fer-1 or a combination of both.
In all cases, the vehicle had the highest BMD values. The iron-dextran mouse model had the lowest BMD in all cases. Total BMD was increased significantly only in the case of the combination therapy with DFO and Fer-1. This was the same result for the measurements of the lumbar and femur region alone. DFO is a Fe chelation molecule used to remove excess Fe and Fer-1 is a lipid peroxidation inhibitor. The combination of both drugs accounts for the total effect seen with the increase in BMD since they act to reduce excess Fe and reduction in ROS.
The accuracy of the iNSiGHT DXA system allows the detection of minor changes in BMD among animal groups within a study. This data supports the pharmacological changes in Table 1. The results of iron overload and reversal via deferoxamine and ferrostatin-1 were further confirmed using micro-computed tomography (micro-CT), H&E, and Masson’s trichrome staining. These other techniques more closely elucidate the mechanism of Fe-overload and the effects on body composition, whereas DXA looks at the global effects. Finally, they are complimentary measurements to have a well-rounded study.
This study concluded that by maintaining Fe homeostasis and inhibiting ferroptosis we can both prevent and treat osteoporosis that is associated with Fe overload. The study also confirmed that the DXA is a precise tool to measure the small changes observed with therapeutic interventions to help treat and prevent human diseases. This highlights the importance of the system in applications for monitoring novel therapies to assess drug safety and effectiveness. This expands into exploring the toxicologic effects of therapy
References
1. Tu, K. N. et al. Osteoporosis: A Review of Treatment Options. vol. 43 (2018).
2. Balasubramanian, A. et al. Risk of subsequent fracture after prior fracture among older women. Osteoporosis International 30, 79–92 (2019).
3. Wright, N. C. et al. The recent prevalence of osteoporosis and low bone mass in the United States based on bone mineral density at the femoral neck or lumbar spine. Journal of Bone and Mineral Research 29, 2520–2526 (2014).
4. Miller, C. J., Rose, A. L. & Waite, T. D. Importance of iron complexation for fenton-mediated hydroxyl radical production at circumneutral pH. Front Mar Sci 3, (2016).
5. Balogh, E. et al. Iron overload inhibits osteogenic commitment and differentiation of mesenchymal stem cells via the induction of ferritin. Biochimica et Biophysica Acta – Molecular Basis of Disease 1862, 1640–1649 (2016).
6. Stockwell, B. R. et al. Ferroptosis: A Regulated Cell Death Nexus Linking Metabolism, Redox Biology, and Disease. Cell vol. 171 273–285 Preprint at https://doi.org/10.1016/j.cell.2017.09.021 (2017).
7. Jiang, Z. et al. Iron overload-induced ferroptosis of osteoblasts inhibits osteogenesis and promotes osteoporosis: An in vitro and in vivo study. IUBMB Life (2022) doi:10.1002/iub.2656.
8. Naot, D. et al. Reduced bone density and cortical bone indices in female adiponectin-knockout mice. Endocrinology 157, 3550–3561 (2016).
9. Yao, G. Q., Troiano, N., Simpson, C. A. & Insogna, K. L. Selective deletion of the soluble Colony-Stimulating Factor 1 isoform in vivo prevents estrogen-deficiency bone loss in mice. Bone Research 5, (2017).
